Definition
Respiratory emergency is one in which normal breathing stops or in which breathing is reduced so that oxygen intake is insufficient to support life.
Artificial respiration is a procedure for making air to flow into and out of a person’s lungs when his natural breathing is inadequate or ceases.
The breathing process
Natural breathing is accomplished by increasing and decreasing the capacity of the chest and the lung. Atmospheric air being under pressure, rushes in and out with the increase and decrease of chest space.
During the inhalation phase of breathing (inspiration), the muscles of the chest lift the ribs, expanding the chest. At the same time the diaphragm contracts and descends toward the abdomen. In this way, the chest cavities increased in size and air flows in. When all muscles relax, the ribs and diaphragm resume their normal position, the chest cavity becomes smaller, and air flows outward. In all manual methods of artificial respiration, the objective is to cause an alternate decrease and increase in size of the chest cavity. When this is done, air flows in and out if there is no obstruction.
Causes of Respiratory Failure
A. Anatomical Obstruction
The most common cause of respiratory emergency is interference with breathing caused by the drooping of the tongue back and
obstructing the throat. Other causes of obstruction that constrict the air passages are:
- Asthma
- Croup
- Diphtheria
- Laryngeal spasm
- Swelling after burns of the face
- Swallowing of corrosive poisons
- Direct injury caused by a blow
B. Mechanical Obstruction
- Solid foreign objects lodging in the respiratory passage e.g. choking of food
- Accumulation of fluids in the back of the throat (mucous ,blood or saliva)
- Aspiration (Inhalation of any solid or liquid substance)
C. Air Depleted of Oxygen or Containing Toxic Gases
- Asphyxia – Is a condition in which there is a lack of oxygen in the blood and the tissue do not receive an adequate supply of oxygen. It may occur due to decreased oxygen in the air or increased carbon monoxide (CO) or other toxic gases e.g., mining area, sewer etc.
- Explosion hazard -Combustible gases that accumulate in confined spaces where natural or manufactured gases are free
in the air, and are explosive in certain concentrations. The explosion may result if a flame is introduced, if static electricity is discharged or if an electric switch doorbell, telephone or other device is used.
D. Additional Causes of Respiratory Failure are
- Drowning
- Circulatory collapse (shock)
- Heart disease
- Strangulation
- Lung disease e.g. pneumonia
- Poisoning by alcohol, barbiturate, codeine etc.
- Electrical shock
- Compression of the chest e.g. accident
Artificial Respiration and Management of Respiratory Accidents
General Information
- The average person may die with in 4- 6 minutes if his/her oxygen supply is cut off.
- Recovery is usually rapid except in case of carbon monoxide poisoning, over dosage of drugs or electrical shock. In such cases, it is often necessary to continue artificial respiration for a long time.
- When a victim revives he/she should be treated for shock.
- A physician’s care is necessary during the recovery period.
- Artificial respiration should always be continued until :
-
-
- The victim begins to breath by himself
- He/she is pronounced dead by a doctor or he/she is dead beyond any doubt
-
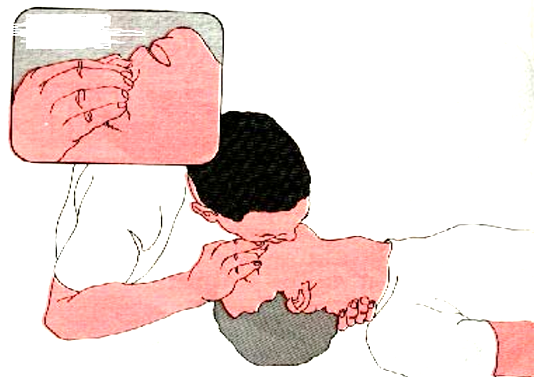
Mouth- to- mouth (mouth- to- nose) method
- Determine consciousness by tapping the victim on shoulder and asking loudly ”Are you OK”?
- Tilt the victim’s head back so that his/her chin is pointing upward. In this case the two procedures can be applied, i.e. head tilt- neck lift and head tilt and chin lift. (fig.1).
- Place your cheek and ear close to the victim’s mouth and nose. Look at the victim’s chest to see if it rises and falls; listen and
feel for air to be exhaled for about 5 seconds. - If there is no breathing, pinch the victim’s nostrils shut with the thumb and index finger of your hand i.e. pressing on the victim’s forehead.
- Blow air in to the victim’s mouth.
Steps of mouth-to-mouth respiration (steps of opening air way)
- Open your mouth wide.
- Take a deep breath.
- Seal your mouth tightly around the victim’s mouth and with your mouth forming a wide open circle and blow into the victim’s
mouth. - Initially give four quick full breaths without allowing the lungs to fully deflate (empty) between each breath.
- Maintain the head tilt and again look, listen, and feel for exhalation of air and check the pulse for at least 5 seconds but
not more than 10 seconds. If no pulse and breath do cardiopulmonary resuscitation (CPR). - If there is pulse and no breath, provide at least one breath every 5 seconds or 12 per minute for adults and this provides sufficient air.
- If the airway is clear only moderate resistance to blowing will be felt.
- Watch the victim’s chest to see when it rises.
- Stop blowing when the victim’s chest is expanded and check for exhalation
- Watch the chest to see that it falls.
- Repeat the blowing cycle.
- For the mouth -to -nose method maintain the backward head -tilt position with the hand on the victim’s forehead and use your other hand to close the victims mouth.
Obstructed airway – unconscious victim
- If you are not getting air exchange, reposition the head and again attempt to ventilate.
- If you still do not get an air exchange immediately turn the victim on his side towards you, resting his chest against your knees
and administer four sharp blows between the shoulder blades. - Place the victim on his back (supine) and spread legs wide apart, straddle his hips or one thigh. This position gives comfort
for the first -aider.
- Open the victim’s airway and sweep with the fingers.
- If the procedures are ineffective, you must repeat the sequence.
Obstructed Air Way – Conscious Victim
The urgency of this situation cannot be over emphasized. Immediate recognition and proper action are essential if the victim has good air exchange with only partial obstruction and is still able to speak or cough effectively. Do not interfere with his attempts to expel a foreign body. If the victim can not speak or cough, shows a distress signal, appears cyanotic or reveals an exaggerated effort to breathe, you must intervene appropriately.
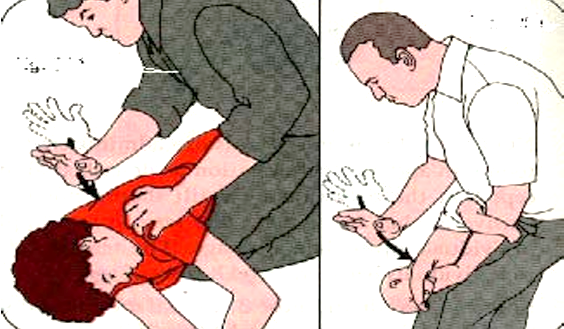
Ingested and Inhaled Objects (Choking)
A small piece of food or a bone (foreign body), may be inhaled in to the wind pipe when eating. Most people on such occasions are able to cough it up at once. Some times, however, this may not be possible and help is needed.
Do not try to hook the foreign body out with your fingers; this is likely to push it further down. Do the following at once.
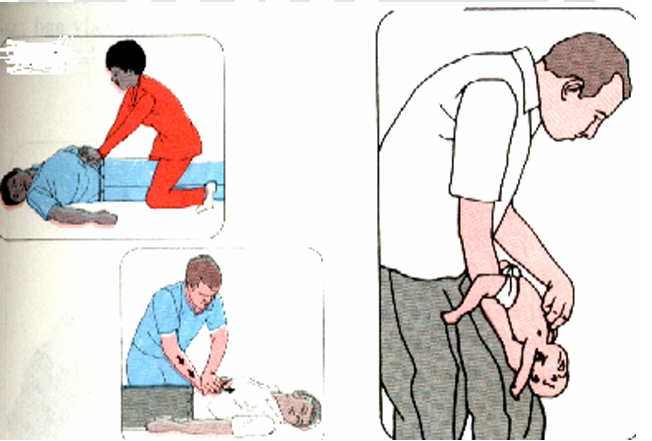

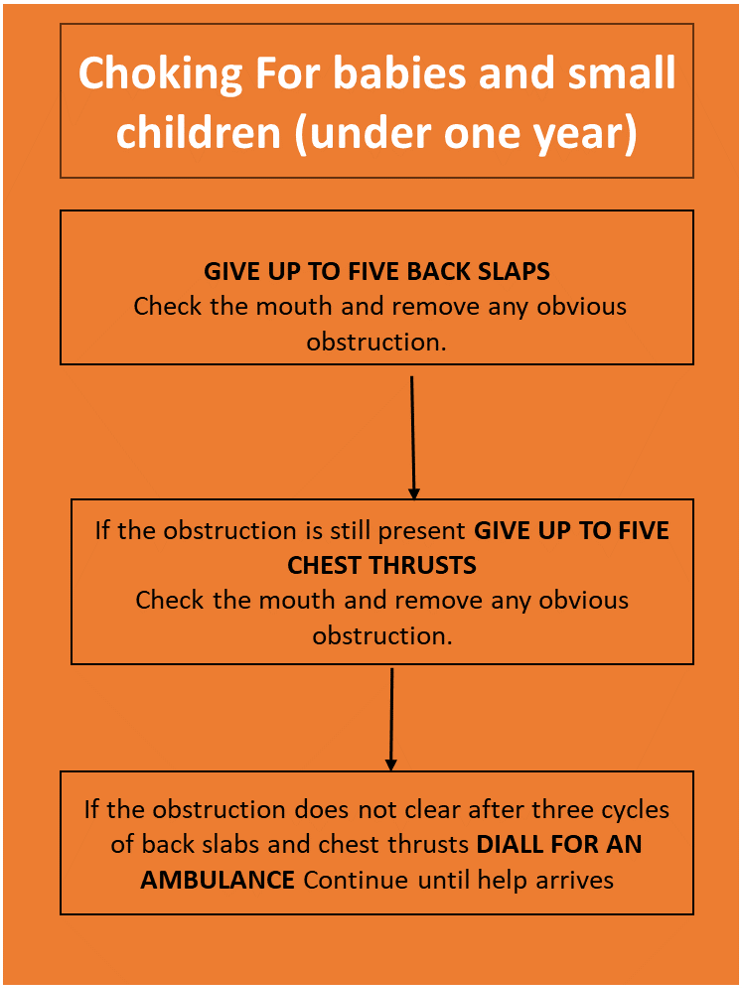
For babies and small children (under one year)
Hold the baby up side down by the feet and smack him firmly between his shoulder blades three to four sharp slaps.
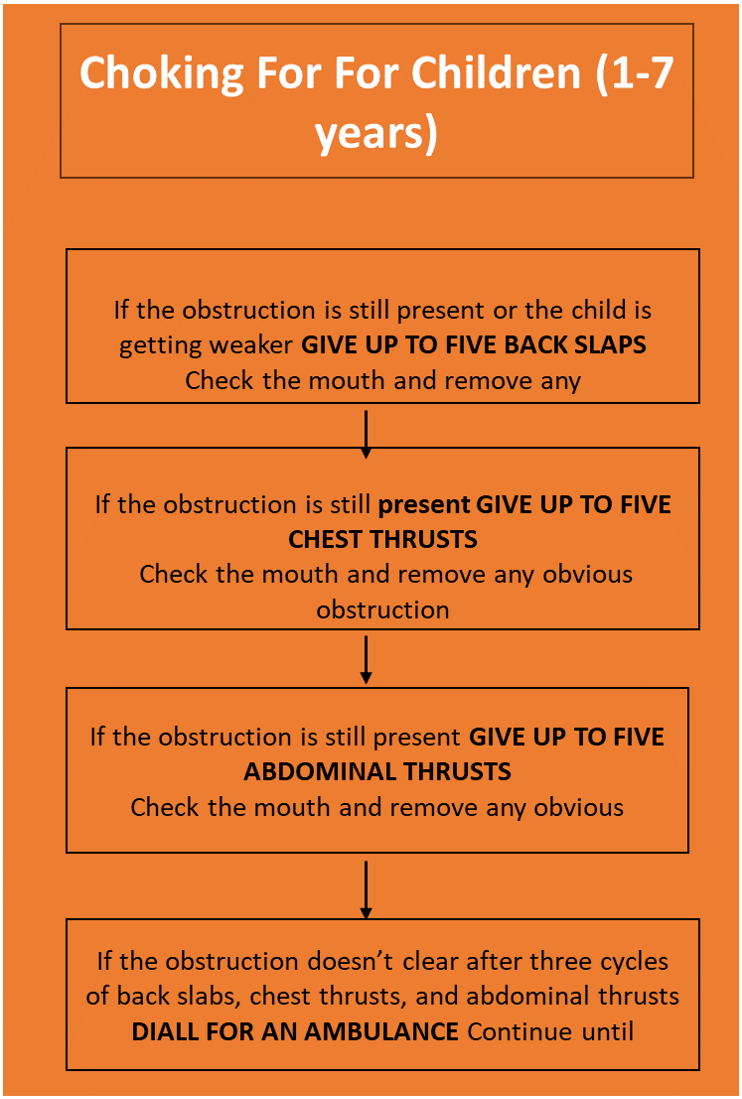
For Children (1-7 years)
Lie the child face down over your knee or arm and smack them sharply between their shoulder blades three to four sharp slaps.
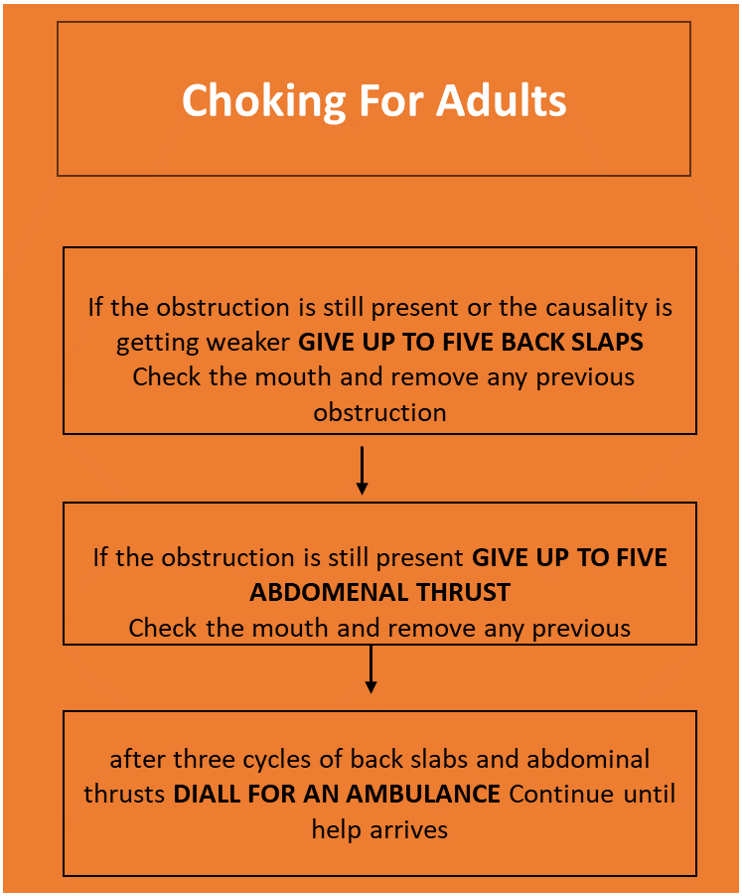
For Adults
Stand behind the patient and grasp them around the chest just under the chest bone (sternum).
Drowning
It is the fourth leading cause of accidental death in the active age groups. Major drowning ranks second in fatality only to motor vehicle accidents; the majority occurs in the recreational play or leisure time activities in developed countries.
The aim of giving first aid for drowning is:
- To restore adequate breathing
- To keep the casualty warm
- To arrange urgent removal to hospital
First aid measure
1. If you are rescuing the casualty from the water to safety, keep the head lower than the rest of the body to reduce their risk of inhaling water.
2. Lay the casualty Prevention of accidental drowning involves: –
- Supervision during swimming.
- Protection of the swimming area and the swimmer.
- Training of the swimming person and life savers.
Mechanical suffocation (Strangulation)
If pressure is exerted on the outside of the neck, the air way is squeezed and the flow of air to the lung is cut off. The main causes
of such pressure are:
- Hanging- suspension of the body by rope around the neck or throat.
- Strangulation- constriction or squeezing around the neck or throat.
Sometimes, hanging or strangulation may occur accidentally- for example, by ties or clothing becoming caught in machinery. Hanging may cause a broken neck; for this reason, a casualty in this situation must be handled extremely carefully.
Recognition (signs)
- A constricting article around the neck
- Marks around the casualty’s neck
- Rapid, difficult breathing; impaired consciousness; grey-Blueskin (cyanosis).
- Congestion of the face, with prominent veins and, possibly, tiny red spots on the face or on the whites of the eyes.
Caution
- Do not move the casualty unnecessarily, in case of spinal injury.
- Do not destroy or interfere with any material that has been constricting the neck, such as knotted rope; police may need it as evidence.
First aid aim and interventions:
The aims are:
- To restore adequate breathing.
- To arrange urgent removal to the hospital
First aid measures are:
- Quickly remove any constriction from around the casualty’s neck. Support the body while you do so if it is still hanging. Be aware that the body may be very heavy.
- Lay the casualty on the ground. Open the airway and check breathing. If he/she is not breathing, be prepared to give rescue breaths and chest compressions if necessary. If he/she is breathing, place her in the recovery position.
Note – Never give an infant plastic material to play with and be certain that mattress covers securely anchored to the bed.
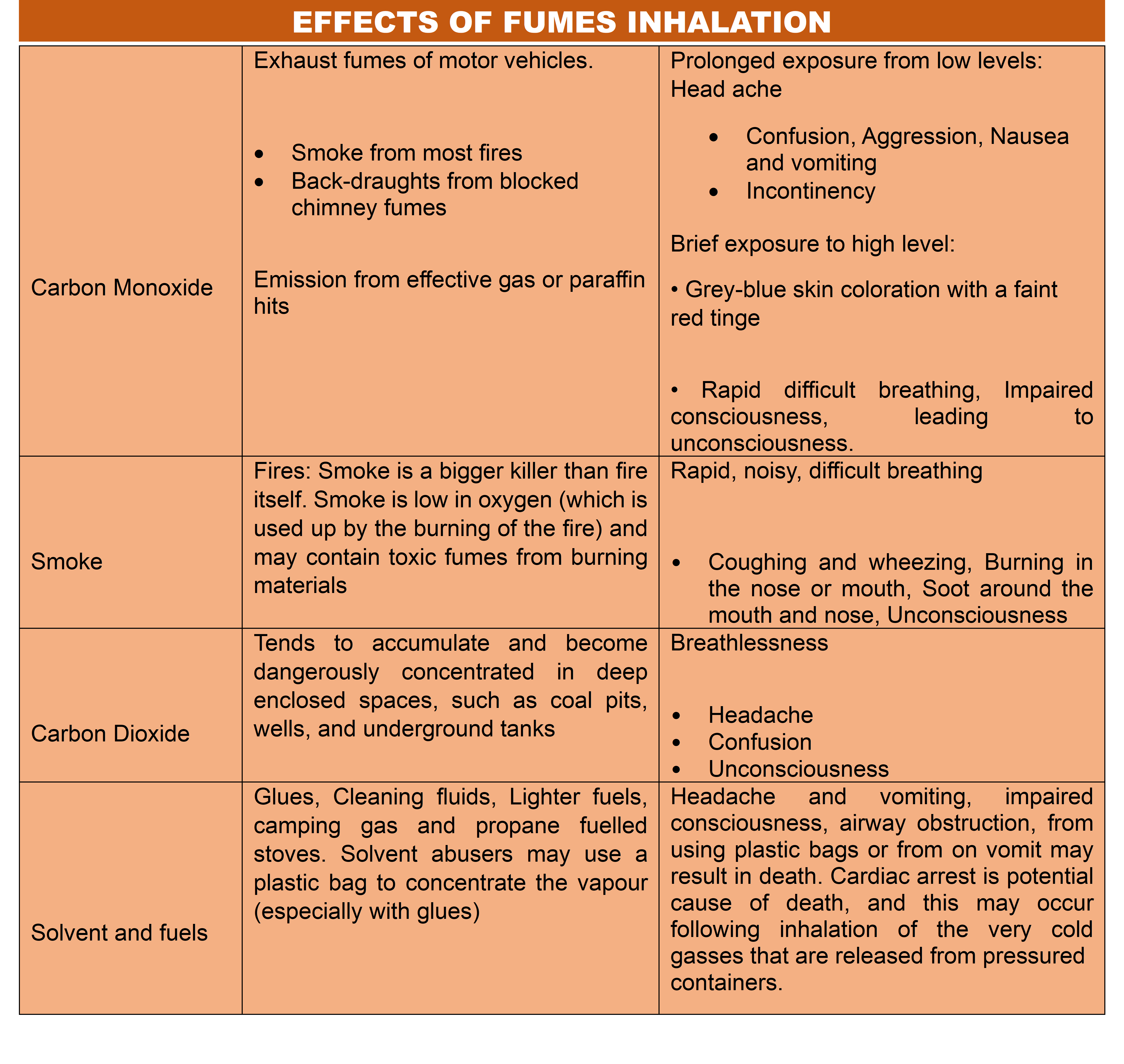
Inhalation of fumes
The inhalation of smoke, gases (such as carbon monoxide), or toxic vapors can be lethal. A casualty who has inhaled fumes is likely to have low levels of oxygen in his/her body tissues and therefore needs urgent medical attention. Do not attempt to carry out a rescue if it is likely to put your own life at risk; fumes that have built up in a confined space may quickly overcome anyone who is not wearing protective equipment.
Inhalation of Smoke
Any person who has been enclosed in confined space during a fire should be assumed to have inhaled smoke. Smoke from burning,
plastics, foam padding, and synthetic wall coverings is likely to contain poisonous fumes. Casualties should also be examined for other injuries due to the fire.
Inhalation of carbon monoxide
Carbon monoxide is a poisonous gas that is produced by burning. It acts directly on red blood cells, preventing them from carrying.
oxygen to the body tissues. If the gas is inhaled into the body in large quantities- for example, from smoke or vehicle exhaust fumes in a confined space- it can very quickly prove fatal. However, lengthy exposure to even a small amount of carbon monoxide- for example, due to a leakage of fumes from defective heater or flue- may also result in sever, or possibly fatal, poisoning.
The aim of first aid is:
- To restore adequate breathing and,
- To obtain urgent medical attention and call the emergency services,
Caution
If entering a garage filled with vehicle exhaust fumes, open the doors wide and let the gas escape before entering.
First aid measures
- HELP: Ask for both fire and ambulance services. If the causality’s clothing is still burning, try to extinguish the flames.
- CASUALITY HANDLING: If it is necessary to escape from the source of the fumes, move the causality in to the fresh air.
- Support the casualty and encourage him/ her to breathe normally. Treat any obvious burns or other injuries.
- Stay with the causality until help arrives. Monitor and record vital signs – level of response, pulse, and breathing.
Furtherly:
- Conditions that allow carbon monoxide to accumulate in closed spaces should be eliminated.
- Never forget to turn of gases cylinder
- Get casualty out door if it so happens
- Open doors and windows and obtain full supply of fresh air
- Resuscitate the casualty if needed
- Do not enter into carbon monoxide suffocated room.
- Be careful of open electrical devices.
Electric current shock
When a person is electrocuted, the passage of electrical current through the body may shock him causing his breathing and even his heartbeat to stop. The electrical current may cause burns both where it enters the body and where it exits the body to go to “earth”. In some cases, the current causes muscular spasms that may prevent a casualty from breaking contact with it, so the person may still electrically charged (“live”) when you come on the sight. Electrical injuries usually occur in the home or workplace, due to contact with sources of low voltage current (opposite). They may also result from contact with sources of high voltage current (below), such as fallen power lines. People who are electrocuted by a high- voltage current rarely survive.
Lightning
A natural burst of electric city discharged from the atmosphere, lightening forms an intense trial of light and heat. The lightening seeks contact with the ground through the nearest tall feature in the landscape and, possibly, through any one standing nearby. A lightning strike may set clothing on fire, knock the causality down, and even cause instant death. Clear everyone from the site of lightening strike as soon as possible.
First aid measures
- Break the contact between the casualty and the electrical supply by switching off the current at the mains or meter point if it can be reached easily. Otherwise, remove the plug or wrench the cable free.
If you cannot reach the cable, socket, or mains do the following:
- To protect your self, stand on some dry insulating material such as a wooden box, a plastic mat, or a telephone directory.
- Using something made of wooden (such as a broom) push the causality’s limbs away from the electrical sources or push the source away from the security.
- If it is not possible to break the contact with a wooden object, loop a length of rope around the causality’s ankles or under the arms, taking great care not to touch him/her, and pull him/her away from the source of the electrical current.
- If absolutely necessary, pull the casualty free by puling at any articles of loss, dry clothing. Do this only as a last resort because the causality may still be “live”.
Warning
- Do not touch the causality if he/ she is contact with the electrical current; he will be “live” and your electrocution.
- Do not use any thing metallic to break the electrical contact. Stand on insulting material and use a wooden object.
- If the causality stops breathing, be prepared to give rescue breathes and chest compression until emergency help arrives.
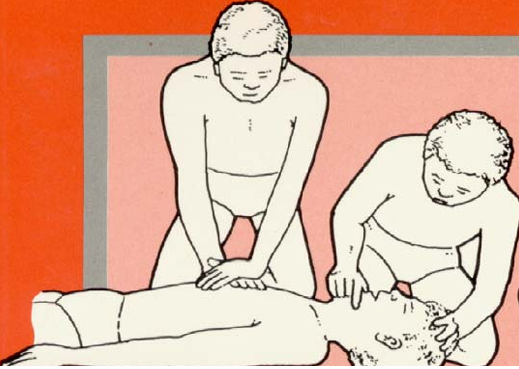
External Cardiac Massage (Cardiopulmonary Resuscitation)
External cardiac message is a combination of artificial respiration and manual artificial circulation. The aim of heart message is to press the heart between the breastbone (sternum) and the backbone (spine) thus literally squeezing blood out of it. Cardio pulmonary resuscitation involves the following steps.
A-Air way opening
B-Breathing restored
C- Circulation restored
D- Definitive therapy
- Lay the patient on a firm flat surface.
- Kneel close to his side, at right angles to him and alongside his chest.
- Press the lower third of his breastbone sharply with the heels of your hands, using pressure from your shoulders. Do not bend your arms at the elbows.
- Check the carotid pulse every few minutes to see if the heartbeat has re started. If you are succeeding the pupils of the patient’s eyes will begin to get smaller. As soon as the patient revives, his neck (carotid artery) and heart recover, pulsate continuously; his/her enlarged pupils shrink to the normal size.